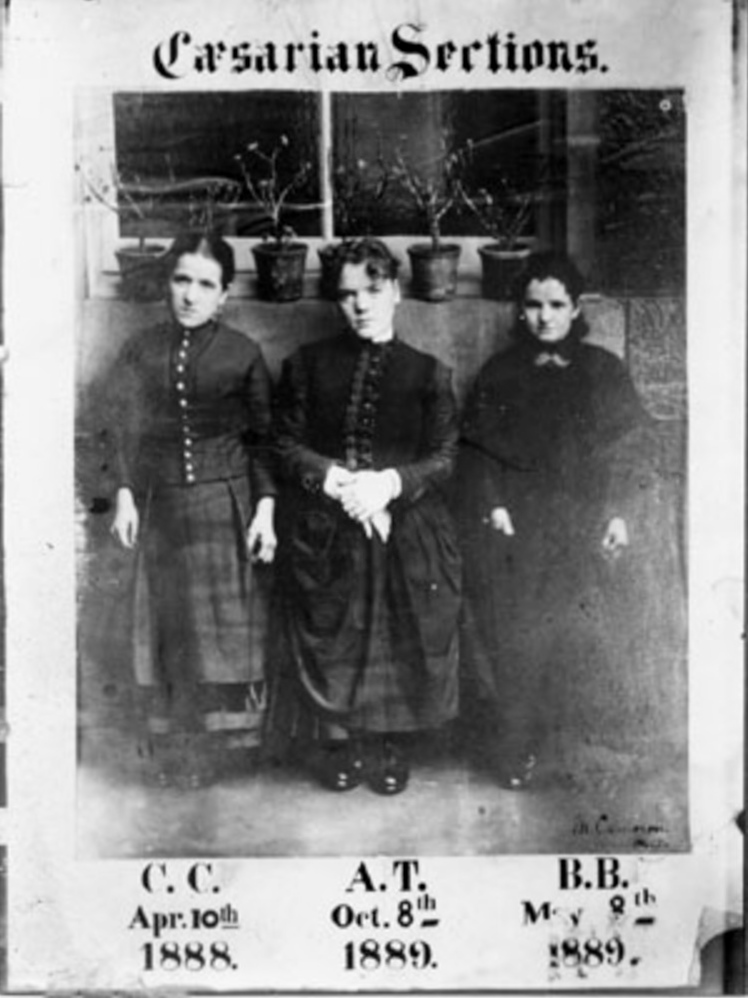
Cameron’s first three patients. Courtesy Glasgow University/Heatherbank Museum of Social Work
Update (October 2022): An updated version of this story appears here in HealthandCare Scotland.
Every woman who now undergoes an elective Caesarian section owes a debt to these wee Glasgow wifies.
They weren’t the first by any means. But they played a key role in establishing that the operation could be carried out safely with both mother and baby surviving.
In medical textbooks they are described as “ricketic dwarfs” who underwent the procedure at Rottenrow – Glasgow Maternity Hospital. The photograph shows the women standing by a window sill at Rottenrow – it was 3 ft 3 in high.
Rickets, a disease caused by vitamin D deficiency through lack of exposure to sunlight or inadequate diet, was rife in Glasgow in the 1880s. It left some women with a deformed pelvis, incapable of delivering a baby and more than likely dying along with their child if they tried.
Obstetrician Murdoch Cameron saw them differently, just as deserving of the fulfilment of motherhood as any other woman.
Caesarian section was still a last resort at this time, along with even ghastlier alternatives – craniotomy and symphysiotomy. Survival rates were as low as one in ten. There was, however, increasing success reported in Europe such as by Max Sänger in Leipzig and Eduardo Porro in Italy.

Murdoch Cameron, pioneer of the elective Caesarian. Courtesy of Glasgow University
This was helped by Simpson’s first use of chloroform as an anaesthetic and Lister’s application of antiseptics in surgery. Cameron had worked under Lister in Glasgow and had closely observed his methods.
Mark Skippen’s PhD thesis provides fascinating background to Cameron’s work and some detail about the women themselves.
The first in April 1888 was 27 years old described as “a little woman, somewhat delicate, and with the appearance of a patient deformed by rickets in a very marked degree.” On arrival, she was already in labour and Cameron, after consulting with colleagues, decided a Caesarian was the only option.
A fire in the operating theatre caused by a bottle of ether catching light delayed the start of the operation and may have helped sterilise the room. It was a resounding success and the mother reportedly christened her son “Caesar Cameron.”
The second woman and her baby also survived. They became a band of mothers – the first two acted as bridesmaids to the third woman who was married at the hospital.
The astonishing success of the operations were reported widely in the Lancet and British Medical Journal. Cameron’s fame also grew, largely through his contributions to international meetings and congresses.
In all he did not do that many – between 10 and 14. Initially he achieved 100 per cent success. Later deaths, probably due to sepsis or other factors rather than the operation, were not reported. Cameron also sterilised all his Caesarian patients by blocking their fallopian tubes, probably out of good intent to spare them another life or death ordeal. It is not clear if he obtained their consent.
What was established in Glasgow was the value of elective Caesarians – women were admitted much earlier with the prospect of a planned operation, not a final desperate attempt to save a woman already exhausted from other attempts to deliver.
At the very least Cameron demonstrated compassion for such pitiable and unfortunate patients and a real desire to help them as best he could. Others had a different view about the voices of women – Simpson was roundly attacked for providing pain relief in labour because their screams of agony were deemed an essential part of God’s will for womanhood.
Religious controversies are still with us. There remains a huge scandal in Ireland over the bizarre reintroduction of symphysiotomies the 1940s as an alternative to Caesarians.
Mark Skippen argues that Cameron’s achievements may have been exaggerated locally but subsequently overlooked internationally.
I wonder what these remarkable women would be thinking now – more than 125 years later when Caesarian sections account for one third or more deliveries in some of the richer countries, increasingly through personal choice rather than clinical necessity.
I suspect their sympathies would be with the 500,000 women around the world who still die every year for want of any basic midwifery or obstetric care.

Slum life for a Glasgow woman and baby c 1910. Courtesy of Glasgow City Council/The Glasgow Story
Glasgow’s contribution to obstetrics has been astonishing. Munro Kerr, Cameron’s assistant and later successor to the chair of midwifery, later refined the Caesarian operation to what it is used today. Ian Donald developed ultrasound now used across the world.
We also have to thank another Glasgow woman in the 1950s who held off going for a pee before a consultation with Donald. The pressure from her full bladder revealed a foetus on the screen. This was the turning point for ultrasound’s transition from a gynaecological to obstetric diagnosis..
My interest in Cameron was triggered by Andrew Calder, a retired professor of obstetrics and lovely guy (he witnessed our daughter Catherine’s entry into the world). He is also a neat historian and his account of Scotland’s contributions to obstetrics is well worth a read.
Further reading:
Obstetric practice and cephalopelvic disproportion in Glasgow between 1840 and 1900 by Mark William Skippen. Glasgow University PhD thesis, 2009.
Categories: case studies, medical and nursing

It’s spelt ‘caesarean’. You’re welcome.
Thanks, Sally.
Both spellings are correct, according to the Oxford English Reference Dictionary.
It’s Caesarean, not Caesarian.
Fascinating read. Thank you for sharing.
“Caesarian sections account for one third or more deliveries in some of the richer countries, increasingly through personal choice rather than clinical necessity.”
Saying the rise in the use of the Caesarian section is due to personal choice is not only offensive to many women who by no means chose to have a section, but it also just inaccurate. The level of research involved in the rest of this article is simply not reflected in that one statement.
Click to access nihms294769.pdf
http://www.childbirthconnection.org/article.asp?ck=10456
“Despite a lot of talk about “maternal request” cesareans, few women appear to be taking this step. Childbirth Connection’s national Listening to Mothers survey of women who gave birth in hospitals in 2011-2012 polled U.S. women about these decisions. Just one percent of women who had had initial (primary) cesareans said that they had planned and carried out surgical birth with the understanding that there had been no medical reason for this procedure.10 Researchers who have looked at this question in other countries have found similar results.11 ……
In other words, there is a change in practice standards that reflects an increasing willingness on the part of professionals to follow the cesarean path under all conditions. In fact, one quarter of the Listening to Mothers survey participants who had cesareans reported that they had experienced pressure from a health professional to have a cesarean.13″
Thanks, Elizabeth. You raise interesting issues. I don’t say the rise in the use of the Caesarian section is due to personal choice. Rates have gone up and an increasing part of that is due to personal choice, as noted in the Yale study you cite. But it is not easy to determine its true significance in this very complex area. As you point out, changing medical attitudes to Caesarians are probably more important. Post-war Ireland demonstrates the appalling damage caused by a prevailing professional paradigm. The wider context is that 500,000 women around the world every year have no choice because they have no access to support from a midwife, birth attendant or obstetrician. And that’s why they die.
And as common sense suggested and research now shows, elective C-section, largely done for medical convenience and profit, leads to compromised health for the baby.
Cutting babies out of women’s bodies is yet another delusional and self-serving medical approach from materialist reductionist mechanistic science. Both mother and baby lose and the doctor wins.
My only observation is the hellish climb up to the Rottenrow from George Street that confronted pregnant women.
Induction Brae
Aw, this was a really good post. Finding the time and actual effort to produce a superb article… but what can I say… I put things off a whole lot and never manage to get anything done.
According to Amand Routh’s publication(s) Cameron Murdoch performed 71 caesarean sections between April 9th 1888 and June 1st 1910.